

Cancer is as much an immune problem as it is a cellular one. Yet one of the immune system’s vital organs is largely absent from that conversation. The thymus is where immature immune cells are trained into functional T-cells, the very cells responsible for recognising and eliminating cancer cells, often long before a tumour forms. For decades, the thymus was dismissed as non-functional and, at times, even disease-causing. As science has since self-corrected, thymic health is now recognised to influence cancer immunity and immunotherapy outcomes. By determining how much immune reserve a patient can draw upon, the thymus may explain why the same therapy can succeed in some patients but fail in others.
A Backdrop on the Thymus Gland
The Thymus Shapes Cancer Immunity and Outcomes
Located between the lungs and overlying the heart, the two-lobed thymus gland follows an unusual life cycle: it grows rapidly until just before puberty, then gradually shrinks and becomes partially replaced by fat in a process called thymic involution. As this shrinkage was once interpreted as a loss of function, the thymus was thought to be expendable. In the early 20th century, the thymus was even wrongly blamed for conditions such as sudden infant death and respiratory failure, leading to its widespread irradiation or surgical removal in millions of people. This was a tragic misstep that later increased the risk of death and cancer.
Only in the latter half of the 20th century was the thymus recognised as an immune organ responsible for educating T-cells, the specialised white blood cells that patrol the body for abnormal cells, including cancerous ones. However, T-cells are not inherently built with such capabilities. T-cell precursors originating in the bone marrow travel to the thymus, where they undergo a rigorous maturation process. Only those that can correctly recognise foreign threats without attacking the body’s own tissues are allowed to mature and enter the bloodstream. The thymus also functions as an endocrine organ, secreting hormone-like peptides (e.g., thymosin, thymopoietin and thymulin) that modulate T-cell and other immune activities.
A healthy thymus, thus, supports a competent T-cell repertoire for immune surveillance. Conversely, as the thymus involutes with age, its output of naïve (new) T cells declines, narrowing immune diversity and contributing to immunosenescence (Figure 1). As a result, the immune system becomes dominated by older, exhausted T-cells. Tumour control then weakens, susceptibility to infection increases, and vaccine response dampens. Far from being a vestigial organ, the thymus is essential to lifelong immune competence by continually renewing the T-cell reserve that underpins our adaptive immunity.
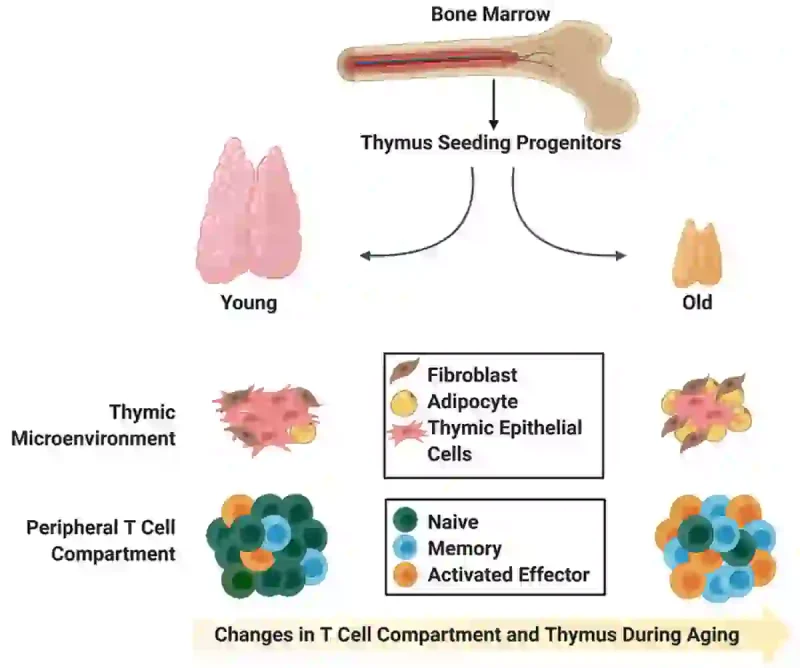
Figure 1. How ageing reshapes the thymus and T-cell repertoire. In young individuals, the thymus continuously produces naïve (new) T cells with a wide range of immune targets, providing strong immune surveillance. With ageing, the thymus gradually shrinks and becomes infiltrated with fat and fibrous tissue, reducing its ability to generate naïve T cells. As a result, the immune system becomes dominated by older memory and activated T cells, thereby losing immune diversity. Source: Singh et al. (2020), Frontiers in Immunology.
If thymic output functions as a form of immune reserve, then the clearest test is what happens when that reserve is removed. Historically, surgical removal or irradiation of the thymus – once justified by the mistaken belief that it was functionless or even pathogenic – was later linked to higher risks of cancer and premature death. In modern clinical practice, thymectomy most often occurs incidentally during cardiothoracic surgery, where partial or complete removal of the thymus is performed to gain access to the heart. Although this removal is not intended to alter immune function, growing longitudinal evidence from the 2025 Mass General Brigham study suggests that even incidental thymectomy increases the risk of cancer incidence and mortality. Among patients with a prior cancer history, thymectomy was also associated with double the rate of cancer relapse. Hence, thymic loss may not only increase cancer emergence, but also weaken longer-term tumour control after completing therapy.
Many factors can place additional strain on the thymus, including stress, ageing, infections, anti-inflammatory steroids and certain cancer therapies (Figure 2). Cytotoxic chemotherapy, in particular, can damage the thymus and reduce its output of T cells. In younger patients, the thymus may partially regrow within a year, but regeneration is age-sensitive and often incomplete. Concerningly, deeper immune profiling shows that even when routine blood counts appear to normalise, the T-cell compartment remains impaired, with reduced T-cell renewal for years after chemotherapy. This has led researchers to propose that long-lasting depletion in the thymic reserve may contribute to several late complications seen in cancer survivors, including increased risks of cancer relapse and secondary cancer.
The thymic reserve becomes increasingly important in the age of cancer immunotherapy. Unlike chemotherapy or radiotherapy, immunotherapy does not directly kill cancer cells; instead, it leverages the immune system’s ability to do so. At the core of this process are T-cells, which carry inhibitory receptors (called immune checkpoints) that act as physiological brakes to prevent excessive immune activation. However, cancer cells can exploit these checkpoints to shut T-cells down. Immune checkpoint inhibitors (or checkpoint blockade immunotherapy) then block this mechanism, thereby restoring the anti-tumour capacity of T-cells. As such, their effectiveness depends on the patient’s T-cell pool (Figure 2).
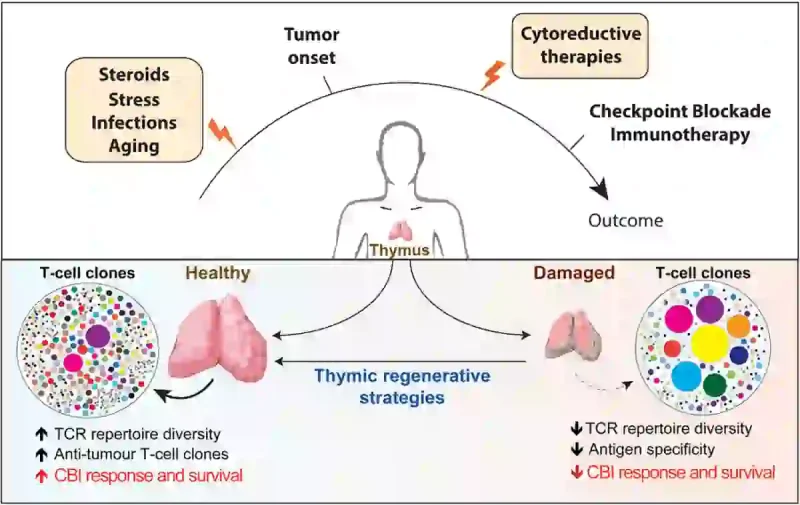
Figure 2. How thymic health shapes immunotherapy outcomes. Physiological stressors such as ageing, infections, steroid exposure and cytoreductive cancer therapies (e.g., chemotherapy and radiotherapy) can damage the thymus and reduce the production of new T cells. This reduces T-cell receptor (TCR) diversity, resulting in poorer cancer control and immunotherapy outcomes. Note: CBI refers to checkpoint blockade immunotherapy, another term for immune checkpoint inhibitors. Source: Cardinale et al. (2020), Frontiers in Immunology.
This poses the question: Does thymic health, which maintains the T-cell pool, influence how well immunotherapy works? This idea was recently tested by Bernatz et al. at Brigham and Women’s Hospital in the U.S. In a 2025 conference report, they used artificial intelligence-based deep learning to develop a “thymic health” score from computed tomography (CT) scans of over 3,400 patients treated with immune checkpoint inhibitors.
Patients with better thymic health consistently fared better. In non-small cell lung cancer, for example, higher thymic health was linked to 35-45% lower risks of disease progression and death, even after accounting for tumour mutational burden and immune evasion capacity. This suggests that, for tumours capable of suppressing T-cells, the thymic reserve could be a deciding factor in clinical outcomes. Similar relationships between thymic health and immunotherapy outcomes were observed for skin, renal and breast cancers, indicating that the effect is not limited to a single tumour type. Patients with healthier thymuses also showed greater T-cell receptor diversity in the bloodstream and within tumours. This receptor diversity matters because it allows T-cells to recognise and target cancer cells with distinct mutations.
As follows, this pioneering study by Bernatz et al. shows that the thymus may set the ceiling for the amount of immune firepower that can be mobilised with immunotherapy. This helps explain why some patients experience long-lasting benefits with immune checkpoint inhibitors, while others, despite having similar tumour profiles, derive far less benefit.
Thymic Support Strategies in Cancer Care
If thymic health shapes immune responsiveness, then strategies aimed at preserving or protecting thymic function may be beneficial to cancer patients and survivors. Ongoing research shows that this is, indeed, possible with several thymic regenerative strategies.
For one, pharmacological expansion of the T-cell pool with interleukin-7 (IL-7) appears promising. IL-7 is a cytokine vital for T-cell survival and fitness. Early human trials of recombinant IL-7 managed to expand T-cell numbers and receptor diversity, highlighting its potential for aiding cancer immunotherapy. Indeed, a recent phase II clinical trial in 2025 combined IL-7 with atezolizumab (an immune checkpoint inhibitor) in patients with advanced urothelial cancer and found the approach to be well tolerated, with clear expansion of the T-cell pool. Importantly, complete tumour disappearance occurred in 10.5% of patients receiving the co-therapy, compared with 4.8% with atezolizumab alone.
Other strategies aim to support the thymus more directly by acting on its structural and hormonal environment. One example is keratinocyte growth factor (KGF), which protects and regulates thymic epithelial cells that nurture T-cells. In humans, a recombinant KGF (palifermin) is already approved for treating oral mucositis (painful ulceration of the mouth lining) during intensive chemo-radiotherapy. Clinical trials are currently exploring whether palifermin can also aid T-cell recovery. A related approach involves thymosin-α1, a hormone-like peptide shown in clinical studies to improve thymic recovery and T-cell output.
One of the simplest forms of thymic support may be zinc, a micronutrient abundant in seafood and beef. In humans, even mild zinc deficiency can impair T-cell function in part because thymulin (a peptide hormone involved in T-cell maturation) is zinc-dependent. As follows, zinc supplementation has been shown to restore thymulin activity and T-cell function in individuals with deficient or suboptimal zinc status. More recently, a 2025 clinical trial reported that zinc supplementation increased lymphocyte count (including T-cells) and thymic output of T-cells in patients recovering from immunosuppressive cancer therapy (Figure 3).
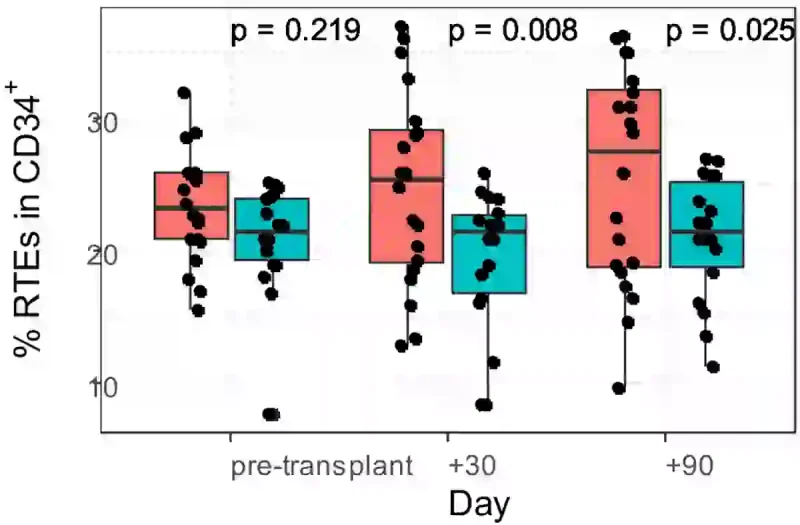
Figure 3. Zinc supplementation supports thymic T-cell recovery after stem cell transplantation, an immunosuppressive procedure, in patients with multiple myeloma (a type of bone marrow cancer). This panel shows the percentage of recent thymic emigrant (RTE) CD4⁺ T-cells – newly produced helper T-cells that reflect thymus activity – measured before transplantation and at 30 and 90 days afterwards. Patients receiving zinc (red) showed a clear increase in newly generated T-cells at both follow-up time points (p < 0.05), whereas the placebo group (blue) did not. Source: Nikoonezhad et al. (2025), BMC Immunology.
Although evidence remains preliminary, complementary approaches such as organotherapy and phytotherapy have also been explored as potential ways to support thymic function. Organotherapy refers to the use of organ-derived extracts or peptides for health support. Given that thymic peptide hormones (e.g., thymosin-α1 and thymulin) aid T-cell maturation and immune regulation, thymus extracts may confer similar immunomodulatory benefits. In fact, early clinical studies suggest that thymus extracts can improve T-cell function and other immune parameters in individuals with immune dysfunction or recurrent infections.
Phytotherapy (phyto- means plant-related) offers another promising avenue. In preclinical studies, certain plant compounds have been found to protect the thymus from inflammatory or oxidative damage. For example, resveratrol delayed thymic shrinkage in mice with premature ageing, while curcumin preserved thymic structure in mice with chemotherapy-induced immune injury. Similar thymus-protective or immune-restorative effects have been reported for quercetin, green tea polyphenols and Cistanche deserticola polysaccharides in animal models of immune suppression. However, these preclinical findings can only support biological plausibility rather than proven thymic restoration in humans.
While many thymic support strategies remain experimental, emerging research points to a fundamental oversight in oncology: cancer outcomes are shaped not only by tumour biology, but also by the state of the immune system confronting it. Recognising and preserving thymic health may, therefore, be one overlooked way to improve long-term cancer outcomes.

