

The mRNA vaccine cancer risk, specifically “turbo cancer,” is not supported by population-level data. While rare case reports document rapid cancer progression after COVID-19 vaccination in genetically susceptible individuals, large registry studies show no vaccine-driven cancer surge. Any observed rebounds in cancer diagnoses are more consistent with pandemic-related disruptions to screening and treatment.
The mRNA vaccine cancer risk, specifically “turbo cancer,” is not supported by population-level data. While rare case reports document rapid cancer progression after COVID-19 vaccination in genetically susceptible individuals, large registry studies show no vaccine-driven cancer surge. Any observed rebounds in cancer diagnoses are more consistent with pandemic-related disruptions to screening and treatment.While the term “turbo cancer” is not a recognised medical term, it has been used in online discussions to describe reports of unusually aggressive cancers appearing shortly after COVID-19 vaccination. Regardless of its existence, turbo cancer has turned into a highly polarised topic. Some individuals are convinced it causes a hidden wave of vaccine deaths, while public health experts largely dismiss it as misinformation unsupported by data. Who is right, then? This answer is not a straightforward one. It demands a careful, objective evaluation of the evidence on both sides, and the answer may not fit neatly into a simple “yes” or “no.”
Does “Turbo Cancer” Exist?
One of the most sobering and cited medical cases of a possible turbo cancer involves Michel Goldman, MD, PhD, an immunology professor long known for championing vaccine research. In 2021, Goldman was diagnosed with angioimmunoblastic T-cell lymphoma (AITL), a rare cancer of follicular helper T cells (Tfh cells) in the lymph node. Facing imminent chemotherapy, Dr Goldman chose to receive an mRNA booster vaccine to ensure maximum protection against COVID-19 before his immune system became suppressed. At the time, Dr Goldman was 66, placing him at high risk amid a surge of new COVID-19 variants.
Within weeks, however, follow-up scans revealed an unusually rapid spread of lymphoma. New lesions had appeared on the right side of the body where the booster shot was injected (Figure 1). Before the booster, the cancer had been limited to his left side only. Troubled by the pattern and timing, Dr Goldman and colleagues published the case in a reputable academic journal, titled “Rapid Progression of AITL Following BNT162b2 mRNA Vaccine Booster Shot.” It was arguably the first scientific report describing a unique case of turbo cancer, where the cancer suddenly accelerates after vaccination in an uncanny and unusual pattern.
As mRNA vaccines are known to activate Tfh cells to drive antibody responses, Dr Goldman and colleagues theorised that this immune stimulation might accelerate cancer growth in individuals whose Tfh cells are genetically unstable. In his case, two mutations commonly linked to lymphoma (i.e., RHOA G17V and TET2) were present in his cancer cells. Supporting this hypothesis, previous mouse studies demonstrated that when both mutations co-exist, exposure to an immune stimulant (i.e., sheep red blood cells) was enough to trigger lymphoma development. Although the stimulant used was not a vaccine, it was the RNA contained in the sheep’s red blood cells that served as the immune stimulant. Since mRNA is a form of RNA, the experiment provides a biologically relevant parallel.
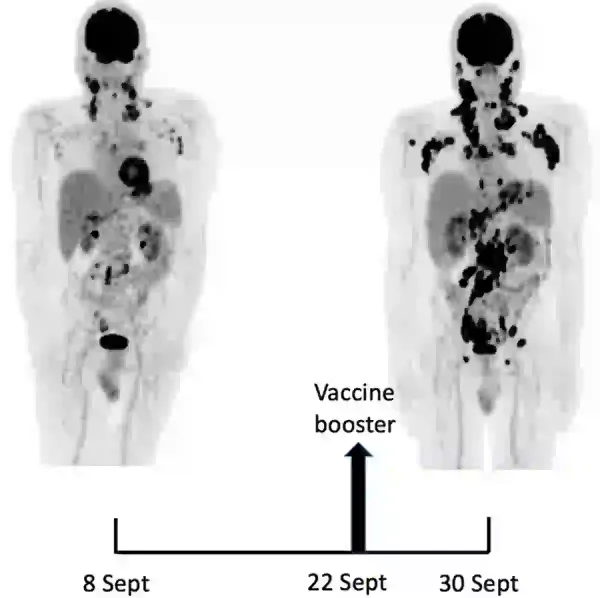
Figure 1. Imaging scans of Dr Goldman before and after his COVID-19 vaccine booster shot. The black spots show areas of active lymphoma. The scan on the left (8 September 2021) shows limited disease mainly under the left arm, while the scan on the right (30 September 2021), taken just over a week after the booster shot, shows many new spots on both sides of the body, indicating rapid spread of lymphoma. Source: Goldman et al. (2021), Frontiers in Medicine
Of course, Dr Goldman also considered the alternative possibility that his lymphoma would have progressed regardless of vaccination. Still, given the temporal (time between booster shot and unprecedented cancer progression), spatial (alignment between vaccine injection sites and tumour spread), and theoretical (biological plausibility) factors, he argued that it would be equally unscientific to dismiss the case as a mere coincidence.
Following Dr Goldman’s publication, a few individuals reached out to share similar stories. At least two have reported that their close relatives developed lymphoma soon after receiving a COVID-19 vaccine. “Again, these could be coincidences,” a journalist noted after interviewing Dr Goldman, “or maybe they are the second and third data points in a growing set.”
Although many studies have evaluated the effectiveness of COVID-19 vaccines in cancer patients, showing generally lower effectiveness than in healthy individuals, far fewer have examined vaccine safety. One meta-analysis that did so pooled 15 studies on blood-related cancers (including lymphomas) and reported no difference in adverse event rates between cancer and non-cancer groups. Still, the total sample size in this meta-analysis was only 2,000 participants, which is too small to detect rare events. If an adverse event occurs in just 1 out of 10,000 people, detecting it with a statistical significance of 95% chance (p < 0.05) would require at least 30,000 participants.
Meanwhile, several published case reports have described new or rapidly progressive lymphoma appearing soon after COVID-19 vaccination, particularly the mRNA vaccine. A 2025 review paper identified at least 15 cases of post-vaccination lymphomas from published case reports or series. The median age of these cases was 50 years, ranging from 20 to 80 years old. Most cases appeared within about two weeks of receiving the mRNA vaccine and involved a less severe lymphoma subtype. Using a standard causality scale, the authors graded the link between vaccination and lymphoma as probable. Besides lymphoma (lymph node cancer), other types of cancers have also been reported to occur or progress rapidly following COVID-19 vaccination in published case reports. These include breast cancer, bladder cancer, myeloma (bone marrow cancer), leukaemia (blood cancer), melanoma (skin cancer), Kaposi’s sarcoma (blood vessel cancer), sarcoma (soft-tissue cancer) and mesothelioma (heart-lining cancer).
(Note: A few case reports have described how COVID-19 vaccination can temporarily mimic cancer spread on medical scans. For example, swollen lymph nodes may appear near a known breast cancer, giving the impression that the disease has spread. In most cases, however, the swelling disappears within a few weeks, indicating it was an immune response to the vaccine rather than true cancer progression. Swollen lymph nodes are a common sign that the immune system is active, which can occur after both infection and vaccination.)
When combined with other anecdotal or unpublished cases, these isolated cases raise the possibility that rapid cancer progression, especially lymphoma, might be a rare adverse event of COVID-19 vaccination, especially in susceptible individuals. If turbo cancer exists, it likely describes such unique instances where immune stimulation by vaccination accelerates a pre-existing or unmasks an underlying cancer. The next question is: has COVID-19 vaccines caused a new wave of cancer at the population level?
What Population Data Do Not Show
While case reports have documented possible instances of turbo cancer, much of the public discourse around it has been distorted. For instance, some bloggers have circulated graphs suggesting an “inflexion point” in cancer mortality around April 2021, coinciding with the rollout of mRNA vaccines in the U.S. The most widely shared versions come from “The Ethical Sceptic,” an anonymous blogger who reprocesses the U.S. Centres for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (CDC’s WONDER) mortality data (Figure 2). While the graphs appear alarming, several methodological issues make them questionable and even unreliable.
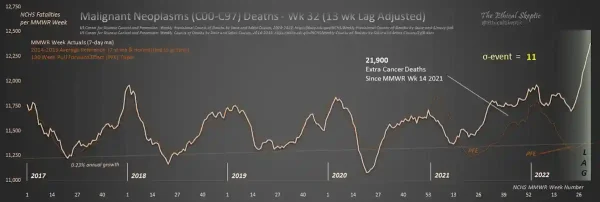
Figure 2. A graph by the blogger The Ethical Sceptic claims there were more than 20,000 extra cancer deaths in the U.S. beginning around April 2021, coinciding with the COVID-19 vaccine rollout. These numbers, however, come from adjustments and assumptions that are not transparent or verifiable. Source: The Ethical Sceptic.
Jeffrey S. Morris, PhD, a professor of biostatistics at the University of Pennsylvania, U.S., pointed out that the huge “20,000 extra cancer deaths” shown in The Ethical Sceptic’s graph are not simply raw counts from the CDC data. They come from layers of adjustments; for example, a “pull-forward effect” assumes that a substantial portion of people who died of COVID-19 would otherwise have died of cancer later. The model also filled in recent weeks with estimated deaths that have not been reported yet. According to Dr Morris, these adjustments are not justified and come across as shady analyses.
When Dr Morris reanalysed the same CDC data without these hidden steps, he did not see signs of a cataclysmic cancer surge. Instead, cancer deaths dipped in 2020 and rebounded modestly in 2021, with about 2,000 excess deaths by early 2022 (Figure 3). To put that in perspective, the U.S. records about 11,500 cancer deaths every week and about 600,000 every year. So, an excess of 2,000 was less than what would normally occur over just two days over a year. In other words, the numbers are far too small to suggest a sudden epidemic of vaccine-driven cancer. Instead, Dr Morris highlighted that the data reflect pandemic-related delays in screening and treatment, which resulted in temporary rebounds in cancer deaths.
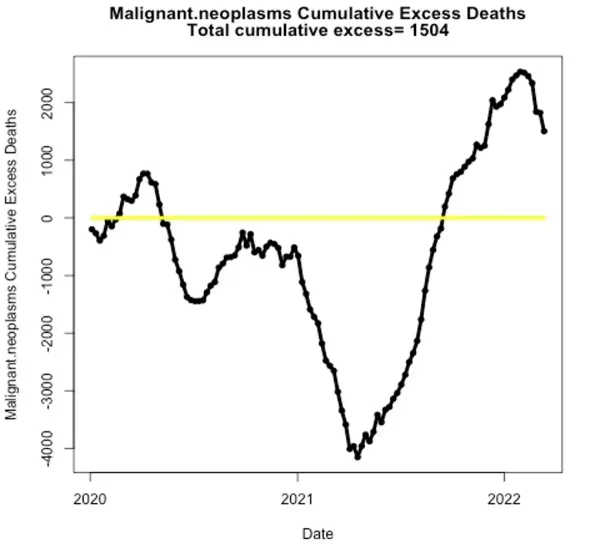
Figure 3. When biostatistician Dr Jeffrey Morris reanalysed the same CDC cancer mortality data, the excess cancer deaths shrank dramatically to only about 2,000 over the entire period. That amount is very small compared with the ~600,000 cancer deaths that occur each year in the U.S., and is consistent with normal fluctuations and pandemic-related healthcare disruptions rather than a vaccine effect. Source: Dr Jeffrey Morris.
A similar claim has circulated using Japanese mortality statistics. In 2024, a now-retracted paper reported an apparent rise in cancer deaths after the third mRNA vaccine dose in Japan in 2022. However, rather than tracking vaccinated individuals, the authors projected Japan’s steadily declining cancer death rate from 2010-2019 into the future and compared that forecast with the actual rates in 2020-2022. In reality, cancer mortality plateaued during the pandemic and even dipped slightly in 2021. As their model assumed the pre-pandemic decline would continue, the observed numbers looked higher than predicted, creating an excess on paper. Put simply, the supposed increase was a mathematical artefact of assuming a continued fall.
This forecasting method, while not inherently wrong, cannot determine why cancer mortality failed to decrease at its previous rate during the pandemic. For instance, pandemic-related disruptions to healthcare, such as delayed diagnoses and treatment interruptions, could plausibly result in a rebound of more advanced cancers by 2022. In fact, this pattern has been observed in other countries (as discussed in the next section). Alternatively, the deviation may reflect short-term reporting variability, since mortality trends rarely follow a perfectly smooth year-to-year trajectory and may temporarily flatten before resuming a longer-term decline. Perhaps the vaccines are indeed responsible, but drawing such a conclusion based on mortality trend forecasting alone is premature without further investigations.
Another debatable data point suggesting the occurrence of turbo cancer nationwide comes from South Korea. Published as a Letter to the Editor (not a peer-reviewed study) in 2025, it linked national insurance data for about 8.4 million people to COVID-19 vaccination records and looked at cancer diagnoses during the following year. Results revealed a higher risk for several cancers (thyroid, gastric, colorectal, lung, breast and prostate) among vaccinated compared with unvaccinated people. This paper is attractive because it is so simple: it tallies cancer diagnoses in the vaccinated vs. unvaccinated group over a year. It is easy to plot the numbers and say “more cancers in the vaccinated group.” However, reality is more complex than that. The simplicity that makes the study catchy also makes it methodologically weak.
- Short follow-up: Cancers take years to develop. A one-year window makes it biologically implausible that vaccination could create new cancers. It is more likely that undiagnosed cancers were found sooner in one group than the other.
- Detection bias: This bias occurs when one group is more likely to have a condition detected because of more frequent healthcare contact or screening. For example, vaccinated individuals often interact more with the healthcare system (appointments and screenings) compared to unvaccinated individuals. This raises the chance of detecting cancers during routine imaging or blood work. As a result, it can create the illusion of a higher cancer rate even if the true underlying rate is the same.
- Confounding factors: The paper did not adjust for major risk factors of cancer, such as smoking, family history or participation in screening programmes. In fact, adjusting for key confounders is a basic requirement in population-level research. Without this step, we cannot be sure whether more people in the vaccinated group simply had more cancer risk factors than those in the unvaccinated group.
These issues mean the South Korean data is best viewed as hypothesis-generating. It does not provide definitive evidence that COVID-19 vaccines cause a drastic surge in cancers. Instead, the results are more plausibly explained by short follow-up, detection bias and unmeasured variables influencing the results. The paper also appeared as a “Letter to the Editor” rather than a full research article. Such letters do not undergo the same level of external peer review or methodological scrutiny as an original research paper.
Another interesting population data comes from Italy involving nearly 300,000 residents, which reported a seemingly paradoxical result: a 23% higher rate of cancer hospitalisation within three months of COVID-19 vaccination, but this association disappeared at 12 months. This pattern is most consistent with detection bias, whereby vaccinated individuals – who tend to engage more with healthcare services – are more likely to have existing cancers detected and managed in hospital settings in the short term. Over a longer follow-up, cancer hospitalisation rates in the unvaccinated group caught up. Moreover, the vaccinated group also had a 58% lower mortality rate than the unvaccinated group. This could mean either (i) that earlier cancer detection and management in the vaccinated group improved survival, or (ii) that the finding reflects healthy vaccinee bias, where vaccinated individuals tend to engage more frequently with healthcare services that improve lifespan.
As the authors of this Italian study concluded, “Given that it was not possible to quantify the potential impact of the healthy vaccinee bias and unmeasured confounders, these findings are inevitably preliminary.” Despite this explicit caveat, the study has been misrepresented online, with attention often focused solely on the short-term 23% increase in cancer-related hospitalisations, while its broader context and longer-term findings are overlooked.
What Population Data Actually Show
Of course, saying there is no sign of a post-vaccination cancer surge does not prove that none exists. If vaccines were truly causing a wave of “turbo cancer,” we would expect to see a noticeable rise in cancer cases beginning in 2021 (i.e., rollout of COVID-19 vaccines) that overshoots pre-pandemic trends.
However, a 2024 study by scientists at the National Cancer Institute (NCI) found that the overall U.S. cancer incidence in 2021 returned to pre-pandemic levels but did not exceed them (Figure 4). In fact, there was no rebound large enough to compensate for the thousands of cancers that went undiagnosed in 2020, when screenings and routine care were disrupted. The only exception was advanced-stage breast cancer, which rose about 9% above expected levels. This statistic likely reflected undetected tumours when mammography services were paused in 2020 and were later diagnosed at a more advanced stage. The overall pattern, therefore, implies that many cancers missed in 2020 were diagnosed later, contributing to the increase we see in recent years.
What makes this study different from the flawed ones discussed earlier is that it is based on real, verified cancer registry data. It does not rely on speculative estimates or models. The research team analysed data from the Surveillance, Epidemiology and End Results (SEER) program, which tracks cancer cases across about half of the U.S. population and is considered the gold standard for national cancer statistics. The methods used were documented, reproducible and peer-reviewed before publication in the Journal of the National Cancer Institute. In short, this is a comprehensive study that tells us what is happening in the population, rather than what might appear in oversimplified or guesswork datasets.
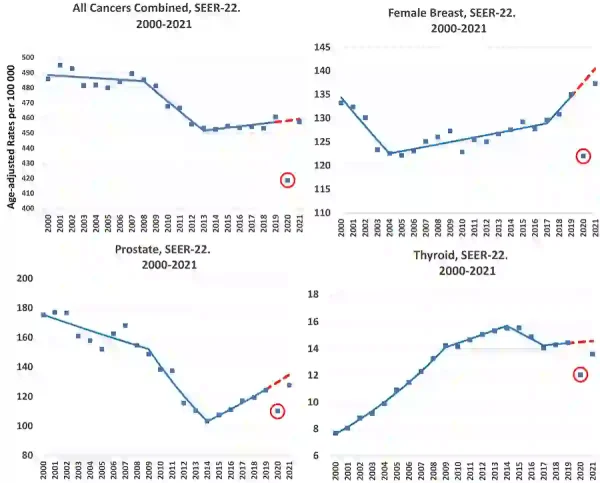
Figure 4. Cancer incidence trends in the U.S. from 2000 to 2021, based on data from the National Cancer Institute. After a sharp drop in 2020 (red circle), new cancer diagnoses in 2021 returned close to pre-pandemic levels but did not overshoot them. In other words, there was no surge or rebound large enough to make up for the cancers missed in 2020. This pattern held true across most cancer types, including prostate, thyroid, and all cancers combined. Source: adapted from Howlader et al. (2024), Journal of the National Cancer Institute.
Similarly, a Europe-wide report estimated that roughly 100 million cancer screenings were missed during the 2020 lockdowns, with 1.5 million fewer cancer patients seen by healthcare providers. About half of those diagnosed did not receive timely treatment, and up to 1 million cancer cases may have gone undetected. For instance, England recorded about 38,400 fewer cancer cases in 2020 (i.e., a 12% decrease), of which about 72% were stage I cancers that went undiagnosed. As a result, some of these cases would reappear at more advanced stages, leading to worse clinical outcomes. Indeed, a 2024 study found that although cancer diagnoses in the U.K. recovered to pre-pandemic levels in 2021, survival rates decreased slightly for several cancers. Another 2025 study reported that stage I breast cancer diagnoses declined in Nordic countries (Denmark, Norway and Sweden) in 2020, followed by a 10% increase in stage II breast cancers in 2021. This suggests some cancers missed in 2020 were detected at later stages. However, there was no drastic overshoot in overall cancer cases above the pre-pandemic trend. The pattern was, thus, one of catching up rather than an epidemic of new cases.
One caveat is that population data arrive with a delay, because registries need time to capture late reports and correct misclassification. For example, the U.S. SEER program uses a standard ~22-month reporting delay. So, cancers diagnosed in 2022 were submitted in late 2024 and only released publicly in spring 2025. Newer analyses incorporating the 2022 SEER data still report about 6.7% fewer cancer diagnoses than expected. However, more recent diagnosis years (2023-2026) remain incomplete. As these data mature in future releases, we will be better equipped to reassess if turbo cancer exists by examining whether any rebound in cancer incidence or death truly overcompensates for the sharp decline observed in 2020.
What About Cancers in the Young?
Much of the discussion about COVID-19 vaccines and cancer also concerns the rise in cancer rates among younger populations, who fall below the recommended age range for cancer screening. In fact, one of the most alarming trends in recent years is the increasing incidence of cancer in young adults, despite cancer being considered a disease of older age. Given that mass COVID-19 vaccination largely coincides with this generation, it is natural to wonder whether vaccination could be a contributing factor, but this is highly unlikely.
The global rise in cancer among younger adults did not begin with the COVID-19 pandemic. Instead, it has been developing gradually over several decades and has only become more apparent in recent years. A 2023 study analysing data from the Global Burden of Disease from 1990 to 2019 reported a 79% increase in the incidence of early-onset cancers (ages 14-49) over that period. The most pronounced rises were observed in breast cancer, followed by nasopharyngeal, prostate, colorectal, stomach and lung cancers. By 2019, early-onset cancers accounted for 3.26 million new cases and 1.06 million deaths worldwide. If current trends persist, the study projects a further 31% increase in early-onset cancer cases by 2030.
A 2024 study examining data from over 217,000 U.S. women diagnosed with breast cancer between 2000 and 2019 provides a closer look at this trend. In 2000, the incidence of early-onset invasive breast cancer was 64 cases per 100,000 individuals. For the next 16 years, this rate rose by just 0.24% per year. After 2016, however, the trend shifted unexpectedly, with incidence rates accelerating at 3.76% per year. By 2019, the rate had reached 74 cases per 100,000 individuals (Figure 5). This pattern is consistent with findings from the abovementioned National Cancer Institute (NCI) study (Figure 4, top right). Given that this inflexion point occurred in 2016, years before the introduction of COVID-19 vaccines, vaccination is unlikely to be responsible for the recent rise in early-onset breast cancer.
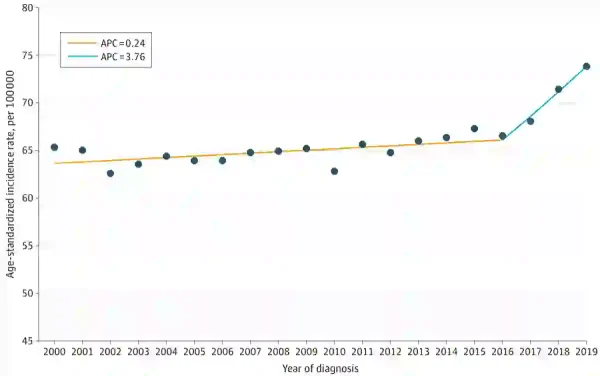
Figure 5. The overall incidence of invasive breast cancer among U.S. women aged 20 to 49 years from 2000 to 2019. The inflexion point occurred in 2016, when the incidence trend increased drastically. Note: APC denotes annual percent changes. Source: Xu et al. (2025), JAMA Network Open.
As discussed in our previous newsletter, researchers attribute much of the rise in early-onset cancers to modern lifestyle changes, including poor diet, alcohol use, smoking, obesity and physical inactivity. Emerging evidence also highlights that the gut microbiota of today’s children is shifting toward a more cancer-prone composition, which may increase the risk of cancer earlier in life. In addition, younger generations are increasingly exposed to endocrine-disrupting chemicals found in plastics, household products and cosmetics. These substances can interfere with hormonal signalling and promote cancer-related cellular processes. When it comes to breast cancer, reproductive factors also play a role. Earlier menstruation, fewer pregnancies and delayed childbirth extend a woman’s lifetime exposure to oestrogen and progesterone, which may promote breast cancer. As more women delay or forgo motherhood, this trend may be contributing to the growing incidence of early-onset breast cancer.
What About the Residual DNA Contamination?
Some have argued that the mRNA vaccines are contaminated with simian virus 40 (SV40) DNA at levels far above regulatory limits. It is important to clarify, however, that this issue does not refer to the SV40 virus itself, but to short SV40-derived DNA sequences involved in certain biomanufacturing processes. As no DNA purification process is perfect, small amounts of residual DNA fragments can remain in biological products like vaccines. For this reason, international guidance sets a conservative safety threshold of 10 ng of residual DNA per dose.
One published paper in 2025 by Speicher et al. quantified residual DNA in Pfizer and Moderna mRNA vaccines using two methods: quantitative polymerase chain reaction (qPCR) and dye-based fluorometry. Using qPCR, all Moderna and most Pfizer mRNA vaccine batches fell below the 10 ng/dose threshold, but two out of six Pfizer batches exceeded that threshold for the SV40 DNA, reaching 23.7 ng/dose. Using fluorometry, Speicher et al. reported much higher total DNA levels of 371 to 6,280 ng per dose, which, if taken at face value, would exceed the threshold guideline by 36 to 627 times (Figure 6, top panel).
However, others caution that fluorometry can overestimate DNA content in mRNA vaccines, because DNA-binding dyes can generate signals from RNA as well. In another 2025 study, Achs et al. showed that extreme fluorometry readings can arise from RNA interference. Using fluorometry, qPCR, fragment analysis and sequencing methods, Achs et al. reported that residual DNA levels remained below 10 ng/dose across 15 mRNA vaccine batches, even with fluorometry (Figure 6, bottom panel). This is because Achs et al. added a DNA isolation step after RNase (an enzyme that degrades RNA) treatment, which reduced residual RNA levels to below 1 ng. Without these steps, the fluorometry readings were inflated. In contrast, Speicher et al. applied RNase treatment alone, without performing DNA isolation or quantifying residual RNA levels, so RNA interference cannot be completely ruled out.
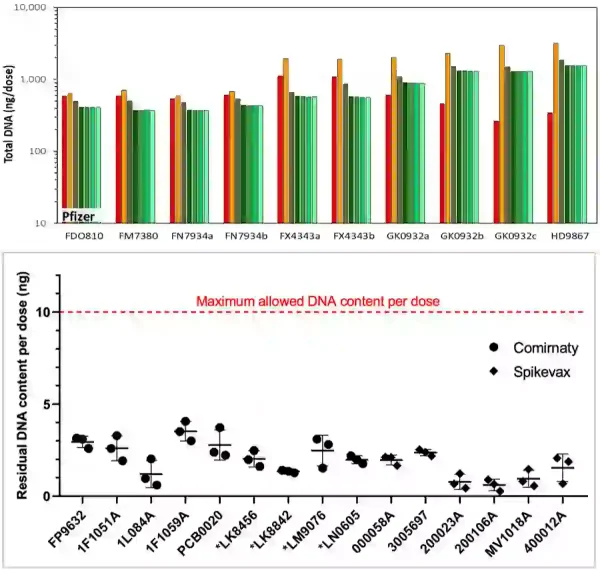
Figure 6. Fluorometry gives very different readings depending on how it is used. Both studies applied RNase treatment to reduce RNA interference before measuring DNA by fluorometry. However, in the top panel (Speicher et al., 2025), fluorometry was performed after RNase treatment but without additional DNA isolation or independent confirmation that RNA levels were fully reduced. In contrast, the bottom panel (Achs et al., 2025) used both RNase treatment and DNA isolation, with residual RNA confirmed to be below 1 ng before fluorometry measurement. Such methodological differences can shift fluorometry readings from over 1,000 ng per dose to below 10 ng per dose, even when measuring the same type of product. Sources: Speicher et al. (2025), Autoimmunity; Achs et al. (2025), NPJ Vaccines.
Official regulators align with the qPCR method. For example, the Australian government has independently tested its mRNA vaccine batches by qPCR, while also noting fluorometry is unsuitable because it “does not meet the requirement for specificity.” That said, while Speicher et al. did acknowledge that the fluorometry dye is nonspecific, they also argued that the standard qPCR method tends to underestimate DNA content, especially with fragmented DNA.
Even with qPCR, Speicher et al. still found that residual SV40 DNA was more than twice the 10 ng/dose threshold in two out of six Pfizer mRNA vaccine batches using qPCR, although what this means clinically is uncertain. This is because the 10 ng/dose limit is a conservative estimate intended to provide large safety margins rather than a direct risk threshold. So, its exceedance does not automatically translate into immediate danger but warrants further investigation into quality control and any potential harm.
Still, critics argue that lipid nanoparticles in mRNA vaccines could theoretically enhance the bioavailability of residual DNA inside cells. So, even a 2-fold increase may be as biologically potent as a 100-fold increase, possibly disrupting genomic stability and fuelling instances of turbo cancers. However, it is equally vital to clarify that lipid nanoparticles enter the cell cytoplasm, not the nucleus, which houses the genome. Cells also have defence mechanisms that keep foreign DNA out of their nucleus; otherwise, our genomes would be constantly altered by DNA from food, microbes or dying cells. As such, authorities such as the U.K. government have stated that they are not aware of evidence showing that residual DNA in mRNA vaccines causes harm.
Even so, both sides are ultimately operating from a theoretical standpoint. More research is certainly needed to determine whether the residual DNA in mRNA vaccines poses any clinically meaningful effects, including carcinogenic potential. Overall, the dispute is less about whether any residual DNA exists than about which measurements best reflect biologically meaningful levels and whether those levels translate into demonstrable harm, for which direct human evidence remains limited.
Weighing the Evidence
What is the verdict on COVID-19 vaccination and turbo cancer? As noted in the introduction, the answer is not straightforward. A small number of carefully documented case reports, such as Dr Goldman’s lymphoma, have shown instances where a pre-existing cancer can progress rapidly after vaccination. Similar case reports exist for lymphomas and other cancers, suggesting that such effects, while real, are highly individualised and not generalisable.
In fact, population-level data tell a different story. Cancer diagnoses worldwide fell sharply in 2020 due to disruptions in healthcare services, followed by a rebound in 2021 and thereafter. However, there was no drastic overshoot that would indicate a vaccine-driven epidemic of cancer. Concerningly, these rebounds often involved cancers being diagnosed at more advanced stages, owing to diagnostic and treatment delays during the first pandemic year. As this rebound coincided with the vaccination rollout, it could create the false impression that vaccines were responsible. Moreover, given the high global vaccination coverage, it is inevitable that most patients diagnosed with cancer from 2021 onward would also have been vaccinated.
That said, it is worth acknowledging a caveat: This 2021 rebound in cancer diagnoses has been attributed entirely to pandemic-related healthcare disruptions. Any concern about a possible vaccination role is immediately labelled as a conspiracy. Playing devil’s advocate, part of that rebound might also reflect other overlapping factors, including the rollout of COVID-19 vaccination. The case reports described earlier leave open the possibility that a tiny subset of cancers, particularly lymphomas, may have been amplified by vaccination. That said, such cases of vaccine-related turbo cancers should be considered exceptions, not the norm.
Most importantly, cancer takes many years, often decades, to develop. Even the strongest and fastest-acting carcinogen, i.e., radiation from atomic bomb exposure, requires years or decades to induce new cancers. It is, thus, biologically implausible that the rollout of COVID-19 vaccines in 2021 could have triggered a wave of new cancer cases within the same year. Rather, any reported instances of turbo cancer are more plausibly explained by the unmasking of undiagnosed cancers or acceleration of pre-existing cancers triggered by immune stimulation in genetically susceptible individuals, such as Dr Goldman’s case. Overall, the totality of evidence indicates that if turbo cancer exists, it likely represents rare, patient-specific reactions, not a widespread effect of vaccination.

